The Demographic Transition in the First World: The Nineteenth Century

Almanac: Globalistics and Globalization Studies Global Evolution, Historical Globalistics and Globalization Studies
The paper is aimed at expanding our understanding of the structure of the demographic transition which took place in Europe in the nineteenth century. In order to achieve this aim we first consider changes in the dynamics and structure of mortality in European countries, and then briefly outline the changes in fertility dynamics. We also investigate the relative extent of the population explosion which Europe experienced as a result of fertility transition lagging behind the mortality transition.
Keywords: demographic transition, fertility transition, mortality transition, Europe, 19th century.
Mortality Transition
Traditional mortality consisted of regular and catastrophic mortality, the latter resulting from separate or combined action of three devastating factors of famine, epidemics, and wars (Vishnevskiy 2005: 45). This type of mortality significantly decreased in Europe in the seventeenth and eighteenth centuries thanks to growing food security, the spread of the New World food cultures, introduction of quarantines, etc.
In the late eighteenth century regular mortality also started decreasing in a number of European countries. The pioneers included the Scandinavian countries, as well as the most developed industrial countries, such as Great Britain and France. Thus, for example, in France the mortality of children under five years old declined from 474 per 1000 (nearly one half!) in 1740–1749 to 306 per 1000 between 1820 and 1830. In Sweden it fell from 344 in the mid-eighteenth century to 250 in the first half of the nineteenth century (Vallin 1991: 56–57).
However, in many countries of the North-western and Central Europe mortality stopped declining in the 1820s – 1830s and remained stable until about the 1870s – in contrast to the Scandinavian countries, where mortality continued to decrease during these decades. Slowing down and / or a complete stop in the decrease of regular mortality was largely due to intense urbanization and the Industrial Revolution (poor quality of life and working conditions, as well as high population density contributed to the maintaining of a high level of mortality from infectious diseases and external causes). In north-western Europe the infant mortality rate correlated with the proportion of the urban population with over 20,000 citizens. In the 1880s three countries with the highest proportion of the urban population – England (and Wales), Belgium, and the Netherlands – had infant mortality rates at 142, 158 and 175 per 1,000, respectively. In Norway and Sweden, where urban citizens constituted less than 14 per cent of the population, these rates were at 96 and 107 per 1,000, respectively (Burnett 1991: 159). In England, the forefront of the Industrial Revolution, mortality reduction stopped for almost 50 years, and resumed only in the last decades of the nineteenth century (Wrigley and Schofield 1981; Caselli 1991).
The last third of the nineteenth century can be called the time of the first ‘medical revolution’ that took place thanks to the works of Pasteur, Koch and other scientists who identified various pathogens, discovered the microbial nature of infectious diseases, and effectively used this discovery in preventive medicine and treatment of infectious diseases (see Table 1).
Table 1. Death rates in Paris by some mortality causes, per 100,000 population, 1876–1905
|
Mortality cause |
1876–1880 |
1881–1885 |
1886–1890 |
1891–1895 |
1896–1900 |
1901–1905 |
|
Typhoid fever |
69 |
88 |
41 |
22 |
19 |
12 |
|
Smallpox |
35 |
21 |
9 |
4 |
5 |
– |
|
Diphtheria |
94 |
88 |
70 |
44 |
13 |
17 |
|
Meningitis |
115 |
110 |
77 |
58 |
45 |
36 |
Source: Biraben 1991: 231.
By the mid-nineteenth century modern ideas about how to combat the spread of cholera began to appear. Effective medical treatment for this disease was not found until much later. However, the incidence of cholera in some areas showed a pronounced decrease when access to infected water sources was blocked. Improving urban water supply systems and the use of sand-based water filtration provided higher-quality drinking water and reduced the incidence of cholera and typhus. Modern systems of sewage and waste management appeared. In 1883 Robert Koch discovered the cholera bacterium, Vibrio cholerae; from this time on bacteriological tests of water started being used for prevention of cholera outbreaks. Drinking boiled water, eating washed fruit and vegetables, frequent hand washing, and other healthy practices became increasingly popular (Bourdelais 1991: 125–128).
Since 1864 Louis Pasteur worked on a disinfection technology which was based on heating products up to a certain temperature for a certain time. The process, known as pasteurization, does not result in product sterilization, but contributes to the destruction of vegetative forms of pathogens without changing the product structure. First of all, pasteurization was (and still is) used for raw milk (see Biraben 1991). The discovery of Pasteur got widespread after the 1890s. It had a particularly pronounced effect on the reduction of infant mortality, as cow milk was widely used for feeding young children (McKeown 1976: 162).
Moreover, the ideas of Pasteur and the British surgeon Lister, as well as other practitioners from European countries, served to develop a complex technology of disinfecting the operating rooms, including thorough hand washing by surgeon and staff, sterilization of all surgical instruments with boiling water, introduction of sterile rubber medical gloves, white coats, etc., which allowed to significantly reduce mortality in patients (Biraben 1991: 227–228).
In the second half of the nineteenth century, but especially from the 1880s – 1890s many European countries (Great Britain, Belgium, Switzerland, France, etc.) approved standards for housing, for example the sizes of rooms, ceiling heights and window sizes, the minimal distance between houses, street width, etc. Slums were gradually rebuilt or demolished (Burnett 1991: 174).
In general, the ‘long nineteenth century’ (from the end of the eighteenth century to 1913) brought tremendous changes to the demographic situation in the European countries in terms of reducing not only catastrophic mortality, but also regular mortality, and increasing life expectancy. We can take France as an example revealing the scale of the changes. Life expectancy increase and mortality reduction were observed in all age groups of French population, especially among children. The risk of death in the age group of 5–10 years decreased by 85 % by 1913 compared to the 1740–1749 level. Mortality declined 75 % among those aged 10–15, 66 per cent for ages 0–5, and about 50 per cent for ages 20–55 years (Vallin 1991: 54). Life expectancy at birth in France increased from 24.7 years in 1740–1745 to 50.4 years in 1909–1913 (Ibid.: 47).
Many other European countries managed to achieve comparable success in combatting mortality. Life expectancy in the world as a whole was only 27 years in 1750 (Biraben 1979: 16). However, after a little more than 150 years many European countries exceeded this rate at least by one and a half times, and some even twofold (see Table 2).
Table 2. Life expectancy at birth on the verge of the World War I in various European countries
|
Country |
Time period |
Life expectancy at birth, years |
|
Denmark |
1911–1915 |
57.7 |
|
Norway |
1911–1921 |
57.2 |
|
Sweden |
1911–1920 |
57.0 |
|
The Netherlands |
1910–1920 |
56.1 |
|
Ireland |
1910–1912 |
53.8 |
|
England and Wales |
1910–1911 |
53.5 |
|
Switzerland |
1910–1911 |
52.3 |
|
France |
1908–1913 |
50.4 |
|
German Empire |
1910–1911 |
49.0 |
|
Italy |
1910–1912 |
46.9 |
|
Finland |
1911–1920 |
46.3 |
|
Spain |
1910 |
41.7 |
Source: Vallin 1991: 47.
The speed of the demographic transition steadily increased with time. In 1750–1850 in England, France and Sweden the annual increase in life expectancy was less than 1 month, while in the 1900s – 1930s it was 5.2 months (Livi-Bacci 2012: 123–124). The Scandinavian countries, the avant-garde of demographic transition in Europe, took 75 years to reduce the infant mortality rate from 150 to less than 50 per 1,000. The countries of Eastern Europe (and many other developing countries), which entered the first stage of the demographic transition much later, took only 20–25 years to achieve the same result (Chesnais 1992: 77).
Fertility Transition
The empirical indicator of the beginning of fertility transition is commonly accepted to be at 10 per cent reduction in fertility rates (Livi-Bacci 2012: 128). The first signs of sustained fertility decline were recorded in the mid-eighteenth century in France. A century later, in 1875–1880, birth rates began to decline in a number of European countries including Sweden, Norway, England, Wales, the Netherlands, Belgium, Finland, somewhat later also Germany, Austria, Czech Republic, Switzerland, and the English-speaking population of Australia and New Zealand. Around 1900 fertility rates started to go down in Poland and the western provinces of Russia, in 1920 also throughout the South-eastern and South-western Europe (Bulgaria, Greece, Romania, Yugoslavia, and Portugal) (Chesnais 1992: 112–113).
In the nineteenth century an essential social constraint on fertility in Western Europe was set by a specific Western European type of marriage characterized by marriage postponement to older ages and a high proportion of people to never marry (see, e.g., Hajnal 1965; Lesthaeghe 1980; Watkins 1981; Coale and Watkins 1986). For example, in 1900 75 per cent of Western European women aged 20–24 were not married – compared to only 25 per cent in Eastern Europe. The share of people who never married was about 10–20 per cent in different Western European countries compared to 5 per cent in Eastern Europe. The average age at first marriage was 26–27 years in Western Europe against 21–22 years in Eastern Europe (Chesnais 1992: 100–101). Notably, in the absence of voluntary birth control an increase in the age of marriage from 18 to 23 years reduces the fertility rate by about 1.5–2 children per woman (Livi-Bacci 2012: 175).
As for the developing world, the first signs of sustainable fertility decline were observed in some countries already in the late 19th – early 20th centuries – especially in Latin American countries with substantial European populations, such as Argentina, Uruguay, and Chile. However, massive fertility transition in the developing world began much later, in the 1960s – 1970s (Ibid.: 174).
Explosive Population Growth in the First World
During the 19th century the European population more than doubled, growing from 180 to 390 million people (McEvedy and Jones 1978: 18). It was a historically unprecedented population increase. For comparison, during the 18th century, a relatively favorable period of the demographic history of the humanity, the population of Europe grew ‘only’ by 50 per cent, from 120 to 180 million. However, even these very impressive figures do not fully reflect the demographic reality because they do not account for the colossal migration from Europe to various settler colonies. For example, the US population increased more than tenfold – from 6 million in 1800 to 76 million in 1900 – largely due to migration of the Europeans (Ibid.: 287). Hundreds of thousands or even millions of Europeans emigrated to Australia (Ibid.: 328), Argentina and Chile (Ibid.: 313–314), Canada (Ibid.: 284), and other countries. Thus, the real growth of the European population far exceeded the level of ‘just’ doubling.
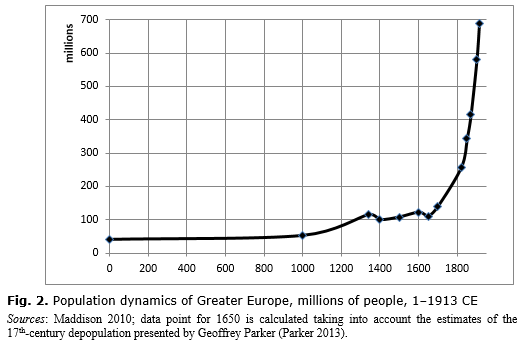
According to the estimates of Angus Maddison, the population of Greater Europe (i.e., the population of Europe, Russia, and settlement colonies in North and South America and Oceania) increased from 257 million in 1820 to 689 million in 1913 (see Fig. 1).

References
Biraben, J.-N. 1991. Pasteur, Pasteurization, and Medicine. In Schofield, R., Reher, D., Bideau, A. (eds.), The Decline of Mortality in Europe (pp. 220–232). Oxford: Clarendon Press.
Bourdelais, P. 1991. Cholera: A Victory for Medicine? In Schofield, R., Reher, D., and Bideau, A. (eds.), The Decline of Mortality in Europe (pp. 118–130). Oxford: Clarendon Press.
Burnett, J. 1991. Housing and the Decline of Mortality. In Schofield, R., Reher, D., and Bideau, A. (eds.), The Decline of Mortality in Europe (pp. 158–176). Oxford: Clarendon Press.
Caselli, G. 1991. Health Transition and Cause-Specific Mortality. In Schofield R., Reher D., and Bideau A. (eds.), The Decline of Mortality in Europe (pp. 68–97). Oxford: Clarendon Press.
Chesnais, J.-K. 1992. The Demographic Transition: Stages, Patterns, and Economic Implications. Oxford: Clarendon Press.
Coale, A. J., and Watkins, S. C. 1986. (Eds.). The Decline of Fertility in Europe. Princeton: Princeton University Press.
Hajnal, J. 1965. European Marriage Patterns in Perspective. In Glass, D. V., and Eversley, D. E. C. (eds.), Population in History (pp. 101–143). London: Edward Arnold.
Lesthaeghe, R. 1980. On the Social Control of Human Reproduction. Population and Development Review 6 (4): 527–548.
Livi-Bacci, M. 2012. A Concise History of World Population. 5th ed. Malden, MA: Wiley-Blackwell.
Maddison, А. 2010. World Population, GDP and Per Capita GDP, A.D. 1–2008. URL: http://www.ggdc.net/maddison.
McEvedy, C., and Jones, R. 1978. Atlas of World Population History. Harmondsworth: Penguin Books Ltd.
McKeown, T. 1976. The Modern Rise of Population. New York, NY: Academic Press.
Parker, G. 2013. Global Crisis. War, Climate Change, and Catastrophe in the Seventeenth Century. New Haven and London: Yale University Press.
Vallin, J. 1991. Mortality in Europe from 1720 to 1914: Long-Term Trends and Changes in Patterns by Age and Sex. In Schofield, R., Reher, D., and Bideau, A. (eds.), The Decline of Mortality in Europe (pp. 38–67). Oxford: Clarendon Press.
Vishnevskiy, A. G. 2005. The Demographic Revolution. 2nd ed. Moscow: Nauka. In Russian (Вишневский А. Г. Демографическая революция. 2-е изд. М.: Наука).
Watkins, S. C. 1981. Regional Patterns of Nuptiality in Europe, 1870–1960. Population Studies 35(2): 199–215.
Wrigley, E. A., and Schofield, R. 1981. The Population History of England, 1541–1871:
A Reconstruction. Cambridge, MA: Harvard University Press.
* This research has been supported by Russian Science Foundation project No 15-18-30063.